
Alcohol After Bariatric Surgery: General Do’s and Don’ts
Bariatric surgery changes more than the size of the stomach. It changes the way the body handles food, fluids, sugar, medication, and alcohol. For this reason, alcohol after bariatric surgery needs to be approached carefully, even when the person is not misusing alcohol and only wants to drink socially from time to time.
This article is not about alcohol abuse. It is about general alcohol use after bariatric surgery, including what patients should understand, what to avoid, and how to make safer decisions after procedures such as gastric bypass and sleeve gastrectomy.
Why Alcohol Feels Stronger After Bariatric Surgery
After bariatric surgery, especially Roux-en-Y gastric bypass and sleeve gastrectomy, alcohol can enter the bloodstream faster than it did before surgery. This means a person may feel the effects of alcohol much sooner, with less alcohol than they previously needed. The American Society for Metabolic and Bariatric Surgery notes that alcohol is absorbed more quickly after bariatric surgery and that patients may have higher alcohol levels for longer after drinking.
In simple terms, one drink after bariatric surgery may not feel like one drink used to feel before surgery. A patient who previously tolerated two glasses of wine may find that one glass now causes dizziness, poor coordination, sleepiness, flushing, or rapid intoxication.
Research discussed in the Bariatric Times article also explains that alcohol pharmacokinetics are significantly altered after both gastric bypass and sleeve gastrectomy, with alcohol levels rising faster and reaching a higher peak than in people who have not had metabolic and bariatric surgery.
Alcohol Is Not Forbidden for Everyone Forever, But It Must Be Treated Differently
Not every patient will be told to avoid alcohol for life. However, almost every bariatric patient should treat alcohol differently after surgery.
The key issue is not only intoxication. Alcohol can also affect weight loss, hydration, blood sugar control, food choices, sleep, liver health, and long-term metabolic goals. Alcohol contains calories but provides no meaningful nutrition. This becomes more important after bariatric surgery because patients have limited stomach capacity and need to prioritise protein, hydration, vitamins, and nutrient-dense foods.
The World Health Organization states that alcoholic beverages contain ethanol, which is a psychoactive and toxic substance with dependence-producing properties. That does not mean every patient who drinks socially has a problem, but it does mean alcohol should be treated as a substance with real physical effects, not as an ordinary drink.
The First Rule: Do Not Drink Alcohol Too Soon After Surgery
The safest general principle is: avoid alcohol during the early recovery and rapid weight-loss phase unless your bariatric team has specifically cleared you.
The early months after surgery are when the body is healing, the stomach is sensitive, food intake is limited, and hydration can already be challenging. Alcohol can irritate the stomach, worsen dehydration, add empty calories, lower inhibitions around food choices, and increase the risk of nausea or vomiting.
Many bariatric programmes recommend avoiding alcohol for a prolonged period after surgery, often during the first months or the first year, but exact advice can vary by surgeon, procedure, medical history, and recovery progress. The Bariatric Times article makes clear that bariatric teams should educate patients about alcohol risks before surgery and refresh that education after surgery because the risk is long-term, not only immediate.
Do: Ask Your Bariatric Team When Alcohol Is Safe for You Personally
The correct timing is not the same for every person. A patient who had a straightforward sleeve gastrectomy, stable blood sugar, no reflux, no liver disease, and excellent nutritional intake may receive different advice from a patient who had gastric bypass, complications, ulcers, diabetes, or a history of alcohol problems.
Before drinking again, patients should ask:
Has my stomach healed enough?
Am I still struggling with nausea, reflux, ulcers, or vomiting?
Am I meeting my protein goals?
Am I taking my supplements properly?
Am I staying hydrated?
Am I still in the rapid weight-loss phase?
Am I on medication that interacts with alcohol?
This is important because alcohol can interact with pain medication, sedatives, antidepressants, sleeping tablets, diabetes medication, and other prescriptions.
Don’t: Test Your Tolerance in Public
A common mistake is assuming that alcohol tolerance after surgery will be the same as before surgery. It usually is not.
Patients who decide to drink after being cleared by their medical team should not test their new tolerance at a wedding, restaurant, party, braai, corporate function, or family event. The first experience after surgery should be approached cautiously, ideally in a safe environment, with trusted people nearby, and with no need to drive.
The reason is simple: alcohol may affect you faster than expected. The ASMBS patient guidance warns that alcohol reaches the bloodstream faster and remains at higher levels for longer after bariatric surgery.
Do: Start Very Small
After bariatric surgery, “moderate drinking” may need to be redefined. A standard serving may be too much for some patients.
A cautious approach would be to take a few sips, wait, and observe how the body responds. Patients should not drink quickly. They should avoid drinking on an empty stomach, and they should stop immediately if they feel lightheaded, flushed, sleepy, unsteady, nauseous, or unusually intoxicated.
This is not about fear. It is about respecting the new anatomy and the new way the body processes alcohol.
Don’t: Drink on an Empty Stomach
Drinking on an empty stomach can intensify the effect of alcohol. After bariatric surgery, this can be even more noticeable because the stomach is smaller and alcohol may pass through more quickly.
Patients should first make sure they have eaten appropriate bariatric-friendly food, especially protein-based food, before considering alcohol. However, they should still follow their bariatric team’s instructions about separating fluids and meals, because many programmes advise patients not to drink fluids immediately before, during, or after meals.
Do: Choose Lower-Risk Options
When a patient has been cleared to drink, the better choice is usually a small, simple drink that can be consumed slowly.
Better options may include:
a small glass of dry wine
a light drink served slowly
a small measured serving rather than a free-poured drink
Riskier options usually include:
cocktails high in sugar
sweet liqueurs
creamy alcoholic drinks
carbonated alcoholic drinks
shots
double spirits
high-alcohol craft drinks
drinking games or rounds
Sugary drinks can add calories quickly and may contribute to unpleasant symptoms in some bariatric patients. Alcohol itself also provides calories without protein, fibre, vitamins, or minerals.
Don’t: Drink Carbonated Alcoholic Beverages Without Medical Guidance
Many bariatric patients are advised to avoid or limit carbonated beverages, especially early after surgery. Carbonation can cause bloating, discomfort, gas pressure, and stomach irritation. This may make drinks such as beer, cider, sparkling wine, champagne, alcoholic seltzers, and mixers like soda or tonic water less suitable for some patients.
This is especially relevant when the patient is still adjusting to smaller portions and slower drinking patterns.
Do: Watch Your Weight-Loss Goals
Alcohol can slow progress after bariatric surgery in several ways.
First, alcohol contains calories. Second, it can reduce self-control around food choices. Third, it may increase snacking. Fourth, it can affect sleep quality, and poor sleep can make weight management more difficult. Fifth, alcohol may displace healthier choices such as water, protein, and planned meals.
The Bariatric Times article notes that substance use after surgery can affect postoperative adherence, including appointment attendance, hydration, supplement routines, food choices, meal planning, portion control, physical activity, and weight outcomes.
For patients who want the best long-term result from surgery, alcohol should never become a regular source of calories.
Don’t: Drive After Drinking, Even After “Only One”
This point is extremely important. After bariatric surgery, a person may be impaired after a smaller amount of alcohol than expected. Because alcohol may be absorbed faster and reach higher levels, “I only had one drink” may not mean the same thing anymore.
Patients should avoid driving after drinking alcohol. They should also be careful with stairs, swimming, exercise, childcare, cooking, and any activity requiring coordination or judgement.
Do: Pay Attention to Changes Over Time
Alcohol sensitivity after surgery is not only an issue in the first few months. Some alcohol-related problems may appear later. The Bariatric Times article explains that the higher-risk period for post-bariatric alcohol problems appears to begin at least around two years after surgery in some research, although some studies observed risk earlier.
Again, this does not mean every patient will develop a problem. But it does mean patients should continue paying attention long after the surgery date.
Warning signs may include:
drinking more often than planned
feeling alcohol more strongly than before
using alcohol to cope with stress
drinking alone more often
choosing alcohol instead of meals
missing supplements or hydration goals because of drinking
weight-loss progress slowing because of alcohol calories
family or friends expressing concern
These signs do not mean a person has failed. They mean it is time to pause, speak to the bariatric team, and adjust.
Don’t: Use Alcohol as a Coping Tool
After bariatric surgery, food can no longer be used in the same way it may have been used before. Some patients feel emotionally unsettled when they lose their old coping mechanism. Alcohol should not become the replacement.
The healthier route is to build new coping tools before they are urgently needed. These can include walking, counselling, support groups, journaling, prayer, hobbies, structured routines, better sleep, or regular check-ins with the bariatric team.
The Bariatric Times article specifically encourages education, monitoring, and healthy coping strategies after surgery because some patients may develop new substance-related difficulties even without a previous history.
Do: Keep Hydration First
Hydration is one of the foundations of recovery and long-term bariatric success. Alcohol can contribute to dehydration, and dehydration can already be a risk after bariatric surgery because patients drink smaller amounts at a time.
If alcohol is used at all, water intake should remain a priority. Patients should avoid drinking alcohol when they are already dehydrated, vomiting, exercising heavily, recovering from illness, or struggling to meet daily fluid targets.
Don’t: Drink While Taking Certain Medications
Alcohol can interact with many medications, including pain medication, sleeping tablets, anxiety medication, antidepressants, sedatives, diabetes medication, and some blood pressure medication. It can also increase the risk of falls, confusion, low blood sugar, stomach irritation, and poor judgement.
Patients should ask their doctor or pharmacist whether alcohol is safe with their current medication list.
Do: Be Honest at Follow-Up Appointments
Patients should feel safe telling their bariatric team whether they drink alcohol and how often. The purpose is not to judge. The purpose is to protect the patient’s health, weight-loss outcome, nutrition, and long-term safety.
Bariatric teams are encouraged to screen for alcohol and substance use both before and after surgery, including long-term follow-up.
A simple honest statement is enough:
“I have started having wine again occasionally. Is that okay with my procedure and my current progress?”
“I feel alcohol much faster now. Is that normal?”
“I am worried that alcohol is affecting my eating plan.”
These conversations are part of responsible aftercare.
Practical Do’s and Don’ts After Bariatric Surgery
Do
Wait until your bariatric team clears you.
Treat alcohol as stronger than it was before surgery.
Start with a very small amount if you are cleared to drink.
Drink slowly.
Avoid driving after any alcohol.
Choose low-sugar, non-carbonated options where appropriate.
Prioritise protein, hydration, vitamins, and follow-up care.
Be honest with your medical team about alcohol use.
Stop if alcohol affects your food choices, hydration, mood, or weight-loss progress.
Don’t
Do not drink during early recovery unless your surgeon says it is safe.
Do not assume your old tolerance still applies.
Do not drink on an empty stomach.
Do not drink quickly.
Do not use alcohol to cope with stress, sadness, boredom, or anxiety.
Do not choose sugary cocktails, shots, or carbonated drinks as a habit.
Do not drive after drinking, even after a small amount.
Do not ignore changes in your relationship with alcohol.
Alcohol after bariatric surgery is not automatically forbidden for every patient forever, but it is never “business as usual.” After gastric bypass or sleeve gastrectomy, alcohol can affect the body faster, more strongly, and for longer than it did before surgery. It can also interfere with hydration, nutrition, weight loss, blood sugar control, and long-term health goals.
The safest approach is simple: wait until your bariatric team clears you, drink very cautiously if you choose to drink, avoid high-risk situations, and keep your health goals first.
References
- American Society for Metabolic and Bariatric Surgery. Life After Bariatric Surgery. The ASMBS notes that alcohol is absorbed more quickly after surgery and that bariatric patients may have higher alcohol levels for longer after drinking.
- Sogg S. Managing Substance Use Issues Before and After Metabolic and Bariatric Surgery. Bariatric Times. 2022;19(8):8-11. This article discusses substance-related screening, alcohol absorption changes after gastric bypass and sleeve gastrectomy, and the need for long-term postoperative education and monitoring.
- World Health Organization. Alcohol Fact Sheet. WHO describes alcohol as containing ethanol, a psychoactive and toxic substance with dependence-producing properties.
- CDC. Alcohol Use and Your Health. CDC explains excessive alcohol use and its health risks.
- MedlinePlus. Alcohol. MedlinePlus explains that alcohol is a central nervous system depressant that can affect mood, behaviour, memory, thinking, coordination, and physical control.

Practical Questions to Ask Before Bariatric Surgery

Bariatric surgery is a major medical decision.
It can support significant weight loss and improve obesity-related health conditions, but it also requires long-term commitment.
That is why your first consultation should not feel rushed.
It should help you understand your options, your risks, your expected results, and your responsibilities after surgery.
The goal is not to ask as many questions as possible.
The goal is to ask the right questions.
A prepared patient usually makes better decisions and has clearer expectations.
What to Bring to Your Bariatric Consultation
Before your appointment, gather the information your bariatric team may need.
This helps the surgeon and support team assess your health properly.
Bring the following if available:
- A list of your current medication
- Your weight history
- Previous diet attempts
- Previous weight-loss medication use
- Diabetes results, if relevant
- Blood pressure history
- Sleep apnoea diagnosis or symptoms
- Reflux or heartburn symptoms
- Details of previous operations
- Medical aid or insurance information
- Your
Continue writing please
personal goals for surgery
You do not need to have every answer before the consultation.
The purpose of the appointment is to help you understand what is medically suitable for you.
Questions About Procedure Choice
Not every patient needs the same operation.
The most suitable procedure depends on your weight, medical history, eating patterns, reflux symptoms, diabetes status, and long-term health goals.
Useful questions include:
- Which procedure do you recommend for me, and why?
- Why would you not recommend the other options?
- Am I better suited to sleeve gastrectomy or gastric bypass?
- How will reflux or heartburn affect the decision?
- How will diabetes affect the decision?
- What weight loss range is realistic for me?
- What are the main risks for my specific health profile?
- What happens if I do not lose enough weight?
- What happens if I regain weight later?
- Will I need a scope, blood tests, or scans before surgery?
A good answer should be specific to you.
If the answer sounds general, ask for more detail.
You should understand why a specific procedure is being recommended before you agree to it.
Questions About Safety and Risk
Bariatric surgery is commonly performed, but it is still major surgery.
You have the right to understand both common risks and serious risks.
Ask your surgeon:
- What are the most common complications?
- What are the serious but less common complications?
- What is my personal risk level?
- How do my age, BMI, diabetes, smoking history, or other conditions affect my risk?
- How do you reduce the risk of blood clots?
- How do you reduce the risk of leaks?
- What symptoms should I watch for after surgery?
- Who do I contact after hours if I am worried?
- What happens if I need to be readmitted?
- How often do complications happen in your practice?
Do not be afraid to ask direct questions.
A responsible bariatric team will explain risks clearly.
They will also explain what they do to reduce those risks.
Questions About Recovery
Recovery is different for every patient, but you should have a clear idea of what to expect.
Ask:
- How long will I stay in hospital?
- When can I walk after surgery?
- When can I drive?
- When can I return to work?
- When can I exercise again?
- What pain is normal?
- What pain is not normal?
- What should I do if I cannot keep fluids down?
- How long will I need help at home?
- When will my follow-up appointments take place?
Many patients focus only on the operation.
Recovery planning is just as important.
Arrange transport, time off work, help at home, and follow-up appointments before surgery.
Questions About Eating After Surgery
Your eating pattern will change after bariatric surgery.
This is not only about eating less.
It is about eating differently.
Ask your dietitian or surgeon:
- What will I eat in the first week?
- When do I move from liquids to soft foods?
- When can I eat normal textured food again?
- How much protein do I need each day?
- How much water should I drink?
- Can I drink tea or coffee?
- When can I drink alcohol again?
- What foods are most likely to cause discomfort?
- What happens if I eat too quickly?
- What should I do if I vomit often?
Eating after surgery is a skill.
You may need to learn smaller portions, slower eating, better protein choices, and proper hydration.
This adjustment takes time.
Questions About Vitamins and Supplements
After bariatric surgery, vitamin and mineral supplements are usually required.
This is especially important after gastric bypass.
Ask:
- Which supplements will I need?
- Will I need them for life?
- How often must I do blood tests?
- Which deficiencies are most common?
- How will I know if I am low in iron, B12, calcium, or vitamin D?
- Can I use ordinary pharmacy multivitamins?
- What happens if I stop taking supplements?
- Are injections ever needed?
- What symptoms should I report?
Do not wait until you feel unwell before checking your levels.
Nutritional deficiencies can develop slowly.
Regular follow-up helps detect problems early.
Questions About Cost and Medical Aid Cover
Bariatric surgery can involve several separate costs.
These may include the surgeon, anaesthetist, hospital, assistant surgeon, dietitian, psychologist, blood tests, scans, and follow-up care.
Ask for a written breakdown.
Important questions include:
- What is included in the quoted fee?
- What is excluded?
- Are hospital fees included?
- Is the anaesthetist included?
- Are dietitian consultations included?
- Are psychologist consultations included?
- Are blood tests included?
- Are follow-up visits included?
- What does medical aid cover?
- Is pre-authorisation required?
- What motivation documents are needed?
- What happens financially if there is a complication?
- What monthly costs should I expect after surgery?
A lower upfront price is not always cheaper.
Good follow-up can prevent expensive problems later.
Questions About Weight Loss Expectations
Patients often want to know how much weight they will lose.
That is understandable.
But no surgeon can promise an exact number.
Ask:
- What is a realistic weight-loss range for me?
- How much weight do patients usually lose after this procedure?
- How quickly does weight loss usually happen?
- When does weight loss slow down?
- What affects my final result?
- What happens if I lose less than expected?
- How do you monitor progress?
- Do you track body composition, or only weight?
- What role does exercise play?
- How do I avoid losing too much muscle?
The scale is only one measure.
Improved blood sugar, better mobility, lower blood pressure, reduced medication, and better sleep may also show progress.
Questions About Weight Regain
Weight regain can happen after any obesity treatment.
It can happen after medication.
It can happen after surgery.
That does not mean the patient has failed.
It means the cause must be assessed.
Ask:
- How common is weight regain after this procedure?
- When does regain usually happen?
- What are the main causes?
- How do you investigate weight regain?
- Can medication be used after surgery?
- Can the stomach stretch?
- When is revision surgery considered?
- Do you offer dietitian support if regain starts?
- Do you offer psychological support if emotional eating returns?
- What early warning signs should I watch for?
The best bariatric programmes plan for weight regain before it happens.
They do not shame patients.
They treat weight regain as a medical and behavioural issue that needs proper support.
Questions About Diabetes, Blood Pressure, and Other Conditions
Many patients choose bariatric surgery because of health problems linked to obesity.
These may include type 2 diabetes, hypertension, sleep apnoea, fatty liver disease, reflux, infertility, or joint pain.
Ask:
- How may surgery affect my diabetes?
- Could my diabetes go into remission?
- Will I need less medication?
- How soon can blood sugar improve?
- Who will adjust my diabetes medication?
- How may surgery affect my blood pressure?
- Will sleep apnoea improve?
- Should I keep using my CPAP machine?
- How will reflux affect my procedure choice?
- How will my liver health be assessed?
Do not stop medication on your own.
Some conditions improve quickly after surgery.
Medication changes must be supervised by your doctor.
Questions About Mental and Emotional Readiness
Bariatric surgery changes eating habits, body size, routines, confidence, and relationships.
Some changes are positive.
Some can feel difficult.
Ask:
- Do I need a psychological assessment?
- What does the assessment involve?
- How does emotional eating affect surgery results?
- What if I binge eat?
- What if I eat when stressed?
- What support is available after surgery?
- Can body image change after weight loss?
- How do patients usually cope with loose skin?
- What if I feel anxious before surgery?
- What if I feel low after surgery?
Mental readiness does not mean being perfect.
It means being honest about habits, triggers, support needs, and expectations.
Questions About the Bariatric Team
Bariatric surgery should not be a once-off transaction.
It should involve a team.
Ask:
- Who will be part of my care team?
- Will I see a dietitian before and after surgery?
- Will I see a psychologist if needed?
- Who manages my diabetes medication?
- Who checks my blood results?
- Who do I contact if I struggle with food?
- Who do I contact if I regain weight?
- How long do you follow patients after surgery?
- Do you offer group support or patient education sessions?
The quality of the team matters.
Surgery is the start of treatment, not the end.
A prepared patient usually makes better decisions and has clearer expectations.
Patient Checklist Before You Decide
Before agreeing to bariatric surgery, make sure you can answer these questions:
- Do I understand the procedure being recommended?
- Do I know why this procedure is best for me?
- Do I understand the risks?
- Do I understand the recovery process?
- Do I know what I will eat after surgery?
- Do I know which supplements I will need?
- Do I understand the cost?
- Do I know my follow-up schedule?
- Do I know who to contact if I have problems?
- Do I understand that long-term results require long-term care?
If you cannot answer these yet, ask for another consultation.
Taking more time before surgery is better than feeling unsure afterwards.
The Bottom Line…
Bariatric surgery can be a powerful treatment for obesity and related health conditions.
But the operation is only one part of the process.
- The best results usually come from careful preparation, realistic expectations, skilled surgery, structured aftercare, and long-term support.
- Before choosing surgery, ask clear questions.
- Understand your options.
- Know your risks.
- Plan your recovery.
- Commit to follow-up.
An informed patient is not being difficult. An informed patient is being responsible.
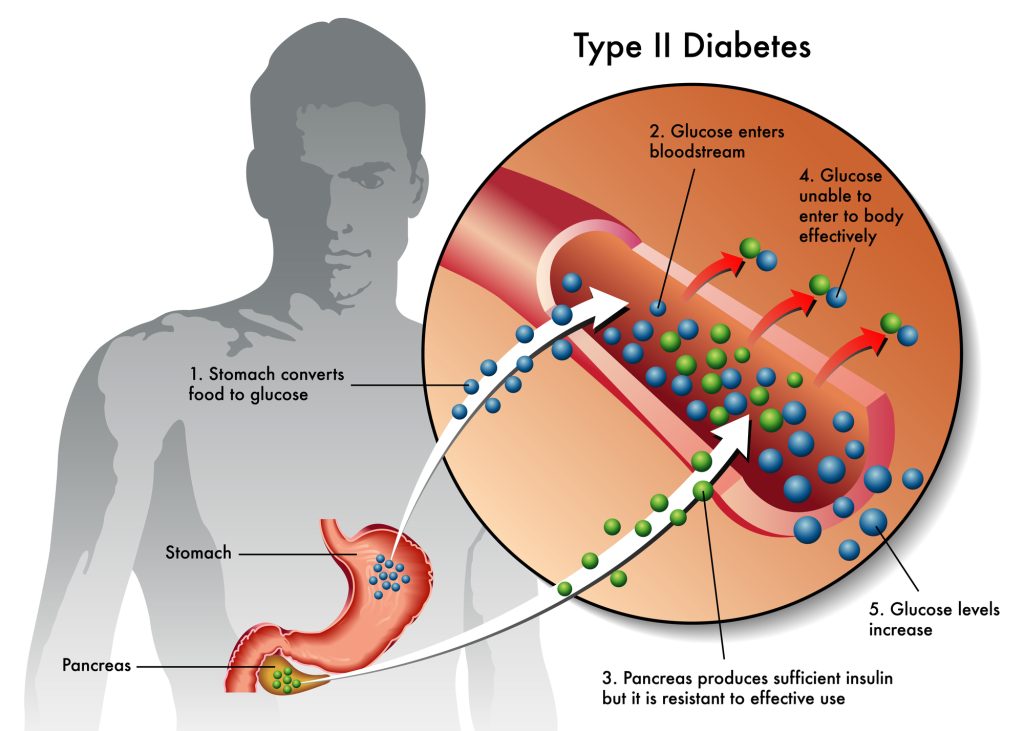
Behind the counter: Glucagon-like peptide-1 receptor agonists for type 2 diabetes
People with type 2 diabetes have a variety of options to manage the condition, including taking prescription drugs and making lifestyle changes. Glucagon-like peptide-1 receptor agonists (GLP-1 agonists) are one option.
In this article, Dr. Maria Prelipcean explains how GLP-1 agonists work, their benefits and risks, and some common side effects.
She also discusses the long-term risks for people who do not manage their type 2 diabetes effectively, along with some lifestyle changes that can make a difference.
What are GLP-1 agonists? How do they treat type 2 diabetes?
A doctor may prescribe GLP-1 agonists to help a person manage their type 2 diabetes.
GLP-1 agonists are a class of drugs that people use to manage type 2 diabetes.
GLP-1 is an incretin, which is one of the gut hormones involved in blood sugar control. GLP-1 agonists help reproduce or enhance the effects of this naturally occurring hormone.
GLP-1 agonists work in several ways, such as by:
- stimulating meal-dependent insulin secretion by the pancreatic beta cells
- decreasing the secretion of glucagon, a hormone that raises blood sugar
- decreasing gastric emptying
- decreasing appetite and reducing food intake by creating a sensation of stomach fullness
GLP-1 agonists may also have some direct effects on brain hunger centers. Since they decrease appetite, they may also help with weight loss.
Their main effect is to decrease spikes in blood sugar after eating. They have a smaller effect on fasting blood sugar levels.
They act mainly on insulin the body produces when a person eats a meal. This means that they are less likely to cause hypoglycemia if a person uses them in isolation, without other medications. However, people more commonly use GLP-1 agonists in combination with other medications for type 2 diabetes.
By themselves, they tend to reduce the glycohemoglobin by 0.5 to 1.2%. Glycohemoglobin is what an A1C test measures. Longer-acting types of GLP-1 agonist tend to reduce A1C levels slightly better.
Beyond managing blood sugar, do GLP-1 agonists have other potential benefits?
GLP-1 agonists do not cause hypoglycemia. This is a significant advantage compared with other antidiabetic drugs.
They also do not cause weight gain. They may even contribute to weight loss, in the range of 1.5 to 3 kilograms. However, this amount varies depending on factors such as lifestyle or the use of other medications.
GLP-1 agonists may also have beneficial effects for heart and kidney health.
Researchers have investigated outcomes for people with type 2 diabetes who take GLP-1 agonists. They found that people who also had heart disease or heart disease risk factors had fewer cardiovascular complications than placebo groups when they took one of the following GLP-1 agonists:
- liraglutide (Victoza)
- semaglutide (Ozempic)
- dulaglutide (Trulicity)
Evidence suggests that all three of these drugs also reduce the progression of kidney disease in people at high cardiovascular risk.
What is the difference between ‘short-acting’ and ‘long-acting’ GLP-1 agonists?
GLP-1 agonists are either “short-acting” or “long-acting,” depending on their dosing schedule and duration of action.
A healthcare provider will recommend a specific medication based on factors such as patient preference, their experience with prior therapies, convenience, and insurance coverage. Currently, no comparative trials demonstrate how choice of medication impacts long-term outcomes.
Short-acting GLP-1 agonists have twice per day dosing. They tend to have a greater effect on after-meal blood sugars and gastric emptying, and a lesser effect on fasting glucose.
One example of a short-acting GLP-1 agonist is exenatide (Byetta).
Long-acting GLP-1 agonists have once-daily or once-weekly dosing. They have a more marked effect on fasting glucose. They may also be slightly more effective at reducing A1C results.
Some examples of long-acting GLP-1 agonists include:
- liraglutide (Victoza), which people take once daily
- semaglutide (Rybelsus), which people take once daily
- dulaglutide (Trulicity), which people take once weekly
- semaglutide (Ozempic), which people take once weekly
- exenatide (Bydureon), which people take once weekly
When do healthcare providers recommend GLP-1 agonists? Can people combine them with other diabetes medications?
The first medication that most people with type 2 diabetes use is metformin. Their doctor may also recommend making lifestyle changes.
However, type 2 diabetes is a progressive condition. Over time, most people will need to use additional therapies. People who experience severe side effects or other issues when they take metformin may also switch to GLP-1 agonists.
GLP-1 agonists may be a better choice when either weight loss or avoiding hypoglycemia is a priority. Healthcare providers may also recommend them for people with elevated postprandial blood sugars.
People with heart disease or heart disease risk factors are also good candidates for this therapy.
In most cases, injectable GLP-1 agonists can reduce blood sugar levels as much as daily insulin injections. People who are interested in GLP-1 agonists but who want to avoid injections could talk to their doctor about an oral form called semaglutide (Rybelsus) that recently became available.
Doctors primarily prescribe GLP-1 agonists in combination with other diabetes medications. The best combination of treatments for any person depends on many factors, including any other conditions they have, their own preferences, and cost concerns.
What are the most common side effects of GLP-1 agonists?
The most common side effects are gastrointestinal. Nausea, vomiting, and diarrhea can occur in many people. Nausea may improve with time and a lower dose. Also, it may occur less often with the weekly types of medication.
Some reports link acute pancreatitis with GLP-1 agonists, but there are not enough data to establish a clear causal relationship. If a healthcare provider suspects pancreatitis, a person should stop the drug and not restart it.
Researchers continue to investigate other possible adverse effects on the pancreas. For example, one group explored whether or not there could be a link between GLP-1 agonists and pancreatitis, as well as pancreatic cancer, but it did not find sufficient evidence of a linkTrusted Source.
Some GLP-1 agonists may cause local skin reactions at the injection site. For example, people using exenatide (Bydureon, Byetta) have reported this side effect.
Hypoglycemia rarely occurs with GLP-1 agonists when a person uses them alone or alongside metformin. However, adding them to insulin-based therapies can increase the risk.
What are the long-term risks of not managing type 2 diabetes effectively?
Diabetes carries an increased risk of complications involving the blood vessels. These are called microvascular and macrovascular complications.
Microvascular complications involve damage to the small blood vessels of the eyes, kidneys, and peripheral nerves. In turn, this leads to retinal damage, chronic kidney disease, and neuropathy.
The damage can be serious. For example, diabetes is one of the leading causes of blindness. It is also the most common cause of end stage kidney disease requiring dialysis.
Treatment makes a difference. A landmark study from 1998 showed that intensive diabetes therapy was associated with a 25% decrease in microvascular complications.
Diabetes also increases the risk of damage to large blood vessels (macrovascular disease) in the heart, brain, and legs. This type of damage increases the risk of heart attacks, strokes, peripheral vascular disease, infections, and amputations.
Managing diabetes effectively by keeping blood sugars within a healthy range makes a big difference in lowering the risk of these complications. It also helps address other risk factors for blood vessel problems.
To manage diabetes, healthcare providers will also encourage people to:
- stop smoking
- lose weight, if necessary
- address high blood pressure, with lifestyle changes or medication
- manage cholesterol levels, with lifestyle changes or medication
People who experience episodes of high blood sugar or severely low blood sugar can also experience serious complications. However, with proper monitoring and an individualized treatment plan, most people can prevent these complications or reduce how often they occur.
What else do people need to know if they are considering starting GLP-1 agonists?
It is important for people to listen to their healthcare provider’s advice when it comes to their treatment plan.
People with a history of pancreatitis should not use GLP-1 agonists. Also, no one with a history of decreased kidney function should use the GLP-1 agonists Byetta or Bydureon.
Based on animal models, people should not use these medications if they have a personal or family history of certain health conditions, including medullary carcinoma of the thyroid or multiple endocrine neoplasia type 2.
Like any other diabetes medication, GLP-1 agonists should be part of a comprehensive individualized treatment plan. The goal of the treatment plan is to keep blood sugar levels in a healthy target range and manage overall health.
Are there any lifestyle changes that may help people with type 2 diabetes?
People with type 2 diabetes should make it a top priority to lower their risk of heart disease. This means following heart-healthy habits, along with managing blood pressure and cholesterol levels.
Depending on the individual, lifestyle changes may include:
- modifying their diet
- quitting smoking
- losing 5–10% of their body weight, for those who have overweight or obesity
- exercising for 150 minutes each week
Healthcare providers may also recommend that people manage cholesterol levels using statin medications.
Self-monitoring of blood sugar levels also improves blood sugar management. Individuals can use a fingerstick method or a continuous glucose monitor.
Seeing a dietitian may help with eating a more healthful diet. A dietitian can recommend an individualized nutrition plan that accounts for a person’s preferences and needs.
In general, when it comes to diet, people may improve their blood sugar management by reducing their intake of carbohydrates, saturated fats, and alcohol and using the diabetes plate method as basic guidance for meal planning.
Medication may also help with weight management in some cases.
When a person has very high blood sugar levels or other symptoms of type 2 diabetes, they need to use insulin. Making lifestyle changes as soon as possible, and sticking with them, may help people prevent the need for additional medication.
Source Credit: https://www.medicalnewstoday.com/articles/glp-1-receptor-agonists-type-2-diabetes?utm_source=ReadNext#lifestyle-changes
Dyspepsia (Indigestion): What It Is, What Causes It, and What to Do
Indigestion is one of those everyday problems that can feel minor… until it keeps coming back. The medical term for indigestion is dyspepsia, which simply means a collection of uncomfortable symptoms in the upper stomach area.

In this guide, we’ll explain dyspepsia in plain language, what to watch out for, and what typically helps
What does dyspepsia feel like?
Dyspepsia often includes one or more of the following symptoms:
- Upper stomach pain or discomfort
- Bloating or feeling uncomfortably full after eating
- Feeling full quickly (even after small meals)
- Belching, regurgitation, or a “sour water” feeling in the mouth
- Heartburn or burning behind the breastbone
- Nausea or vomiting
- Retrosternal (chest-area) burning
A quick note: “organic” vs “functional” dyspepsia
Doctors usually group dyspepsia into two broad types:
Organic dyspepsia means there’s a clear cause, such as:
- Peptic ulcers
- Acid reflux (GERD)
- Less commonly, upper GI cancers
Functional dyspepsia means symptoms are real, but tests don’t show a clear structural problem. It may be linked to diet, stress, and lifestyle.
Dyspepsia is common—but persistent symptoms should be assessed properly so serious causes aren’t missed
Red flags: when indigestion needs urgent medical attention
Some symptoms increase the chance of a serious underlying problem. If you have any of the below, don’t self-treat—see a doctor promptly.
Alarm features include:
- Age 50 or older (especially if symptoms are new)
- Difficulty or pain when swallowing
- Vomiting blood, passing black stools, or any GI bleeding
- Unexplained weight loss
- Iron deficiency (with or without anaemia)
- A palpable abdominal mass
- Severe or persistent abdominal pain
- Regular use of ulcer-causing meds like NSAIDs (e.g., ibuprofen, diclofenac)
- Strong family history of upper GI cancer or relevant genetic syndromes
If you’re under 50 with no red flags: the usual starting approach
When someone is under 50, has no alarm features, and no concerning medical history, management often starts with a “low-risk” pathway.
1) Test for H. pylori
Helicobacter pylori is a common stomach infection that can cause inflammation and ulcers. Recommended non-invasive tests include:
- Urea breath test, or
- Stool antigen test
Important: In high-prevalence settings like South Africa, blood (serology) tests are not recommended because they may not reliably show active infection.
2) Try acid-reducing treatment (PPI trial)
A proton pump inhibitor (PPI) reduces stomach acid and can help symptoms settle. A typical trial is 6–8 weeks.
3) If H. pylori is positive, treat it
If the test is positive, eradication therapy is recommended.
4) Reassess
If symptoms persist or return after initial treatment, the guidance recommends upper endoscopy (a camera test of the oesophagus and stomach).
When is an endoscopy recommended upfront?
If you are 50+, have alarm features, or have persistent symptoms, an upper endoscopy is recommended to look for ulcers, erosions, growths, or other causes.
Practical lifestyle tips that often help (for everyone)
These everyday changes are recommended in all cases of dyspepsia:
- Avoid common trigger foods (often citrus, tomatoes, chocolate, spicy, fatty/fried foods)
- Eat smaller meals more often
- Choose lower-acid foods where possible
- Stay hydrated
- Maintain a healthy weight
- Avoid tight clothing around the stomach
- Elevate the head of the bed if night symptoms are a problem
- Don’t lie down for 2–3 hours after eating (avoid late-night meals)
- Manage stress (breathing exercises, meditation, relaxation)
- Avoid smoking
- Limit caffeine and alcohol
- Avoid fizzy drinks if they worsen bloating
Over-the-counter and prescription options (simple explanation)
Antacids (fast, short-term relief)
Antacids neutralise stomach acid and can help heartburn, indigestion, and bloating. Common ingredients include calcium carbonate, magnesium hydroxide, or aluminium hydroxide.
They can have side effects (like diarrhoea or constipation) and may interact with other medicines—so if you’re using them often, get checked.
Acid suppression (stronger symptom control)
Acid-suppressing medicines reduce acid production and can be very effective.
- PPIs are often first-line for dyspepsia (examples include esomeprazole, lansoprazole, pantoprazole, rabeprazole).
Long-term PPI use should be reviewed with a clinician due to potential risks.- H2 blockers can help mild-to-moderate symptoms (e.g., famotidine, cimetidine, nizatidine). Ranitidine has been withdrawn for safety reasons.
H. pylori treatment and follow-up (the important bits)
Treatment uses combinations of acid suppression + antibiotics (and sometimes bismuth), and the exact regimen depends on local resistance patterns and prior treatment.
Confirming eradication matters: a urea breath test or stool antigen test is used at least 4 weeks after treatment ends to confirm the infection is cleared.
Frequently asked questions (FAQ)
“Is indigestion always caused by acid?”
Not always. Dyspepsia can be linked to reflux/acid, ulcers, H. pylori, certain medications, diet, and stress.
“If a PPI helps, do I still need tests?”
If you have red flags or are 50+, an endoscopy is recommended to rule out more serious issues.
“When should I stop self-treating?”
If symptoms are persistent, worsening, or you’re relying on antacids/acid reducers frequently—or you have any alarm features—get assessed.
Key takeaways
- Dyspepsia is common and often treatable.
- Red flags (especially age ≥ 50, bleeding, weight loss, swallowing problems, anaemia/iron deficiency) should be checked urgently.
- Low-risk patients typically start with H. pylori testing and/or a PPI trial, plus lifestyle changes.
Source Credit: SAJGH_SAGES_dyspepsia_guidance
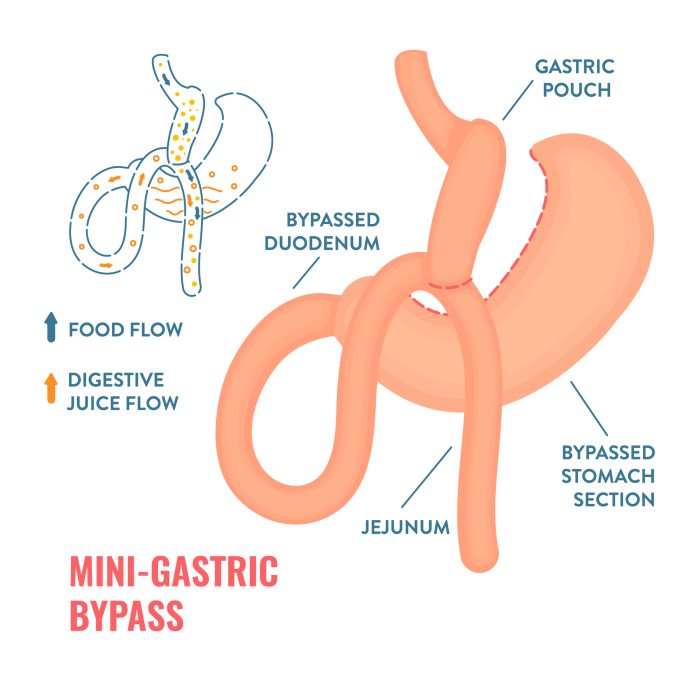
Gastric bypass (Roux-en-Y)
Gastric bypass, also called Roux-en-Y (roo-en-wy) gastric bypass, is a type of weight-loss surgery that involves creating a small, egg-sized pouch from the stomach. The newly created pouch is then connected directly to the small intestine. After gastric bypass, swallowed food goes into this small stomach pouch and then directly into the small intestine, thereby bypassing most of the stomach and the first section of the small intestine.
Gastric bypass is one of the most commonly performed types of bariatric surgery. Gastric bypass is done when diet and exercise haven’t worked or when you have serious health conditions because of your weight.
Roux-en-Y Gastric Bypass
Why it’s done
Gastric bypass is done to help you lose excess weight and reduce your risk of potentially serious health issues, including:
- Gastroesophageal reflux disease.
- Heart disease.
- High blood pressure.
- High cholesterol.
- Obstructive sleep apnea.
- Type 2 diabetes.
- Steatotic liver disease, formerly known as fatty liver disease.
- Stroke.
- Cancer.
- Infertility.
- Urinary incontinence.
- Joint pain.
Gastric bypass is typically done only after you’ve tried to lose weight by improving your diet and exercise habits.
Who is a candidate
In general, gastric bypass and other weight-loss surgeries may be an option for you if:
- Your body mass index (BMI) is 40 or higher.
- Your BMI is 35 to 39.9, and you have a serious weight-related health condition, such as type 2 diabetes, high blood pressure or severe sleep apnea. In some cases, you may qualify for certain types of weight-loss surgery if your BMI is 30 to 34 and you have serious weight-related health conditions.
But gastric bypass isn’t for everyone who is severely overweight. You may need to meet certain medical guidelines to qualify for weight-loss surgery. You likely will have a screening process to see if you qualify.
You must also be willing to make permanent changes to lead a healthier lifestyle. You may be required to participate in long-term follow-up plans that include monitoring your nutrition, your lifestyle and behavior, and your medical conditions.
Check with your health insurance plan or your Medical Aid to find out if your policy covers weight-loss surgery.
Recent Comments